×
Home
Go to course
Go to course
Monthly limit
Initial appointment
Reviews
Clinical Outcomes
Measures
TFI
THI
PSS
GAD
ASQ
HSQ
Why CBT
1-1 CBT for Tinnitus
Tinnitus & Trauma
Autonomic ladder
Tinnitus Trauma
CBT4T Bulletin
Blog
Journey
See us on Facebook
Tinnitus UK
Tinnitus UK
Membership
TinnitusUK Partner
TEP Support
SITREP
First appointment
Using Zoom
Other resources
More
Introduction
Conditions of Use
Mission Statement
History
Testimonials
Privacy Policy and cookies
Free stuff
Introduction
Breath work
Physiological
Negative Thoughts
Cognitive Distortions
Thought records
Professionals
Audiologists
About me
Background
Experience
Development
CBT for Tinnitus E-Programme
Tinnitus E-Programme
×
Home
Go to course
Go to course
Monthly limit
Initial appointment
Reviews
Clinical Outcomes
Measures
TFI
THI
PSS
GAD
ASQ
HSQ
Why CBT
1-1 CBT for Tinnitus
Tinnitus & Trauma
Autonomic ladder
Tinnitus Trauma
CBT4T Bulletin
Blog
Journey
See us on Facebook
Tinnitus UK
Tinnitus UK
Membership
TinnitusUK Partner
TEP Support
SITREP
First appointment
Using Zoom
Other resources
More
Introduction
Conditions of Use
Mission Statement
History
Testimonials
Privacy Policy and cookies
Free stuff
Introduction
Breath work
Physiological
Negative Thoughts
Cognitive Distortions
Thought records
Professionals
Audiologists
About me
Background
Experience
Development
Go to content
×
Home
Go to course
Go to course
Monthly limit
Initial appointment
Reviews
Clinical Outcomes
Measures
TFI
THI
PSS
GAD
ASQ
HSQ
Why CBT
1-1 CBT for Tinnitus
Tinnitus & Trauma
Autonomic ladder
Tinnitus Trauma
CBT4T Bulletin
Blog
Journey
See us on Facebook
Tinnitus UK
Tinnitus UK
Membership
TinnitusUK Partner
TEP Support
SITREP
First appointment
Using Zoom
Other resources
More
Introduction
Conditions of Use
Mission Statement
History
Testimonials
Privacy Policy and cookies
Free stuff
Introduction
Breath work
Physiological
Negative Thoughts
Cognitive Distortions
Thought records
Professionals
Audiologists
About me
Background
Experience
Development
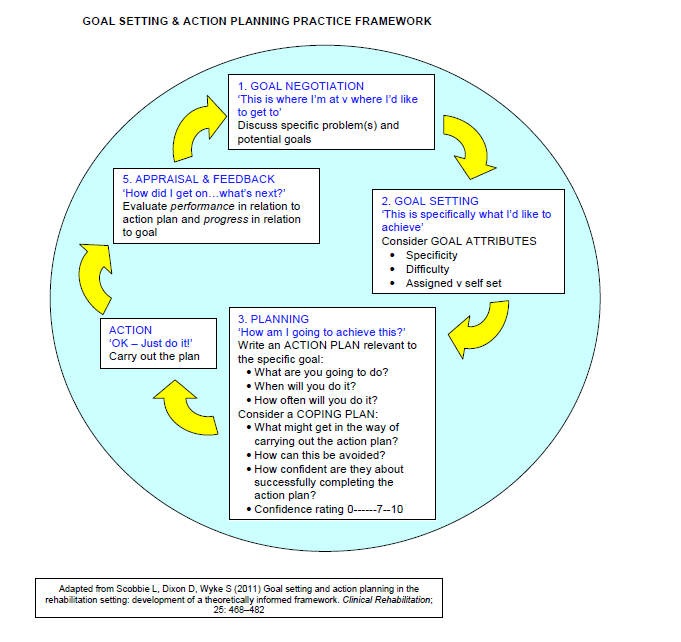
Goal Setting & Action Planning
Date*
Your email*
1. What is your goal?*
2. Is this goal a short, medium or long term goal?*
-
Short term
Medium term
Long term
3. How well do you meet this goal before you begin working toward it? (0 = I don't meet it at all)*
-
10
9
8
7
6
5
4
3
2
1
0
4. What will help you reach your goal?*
5. What are you going to do?*
6. When will you do it?*
7. How often will you do it?*
8. What might get in the way of carrying out your action plan?*
9. How can this be avoided?*
10. How confident are you about completing your action plan on a scale of 0-10 (0 = not at all confident; 10 = very confident indeed)*
-
10
9
8
7
6
5
4
3
2
1
0
Back to content
To use this website you must enable JavaScript.